Videos
The Stealth Invader
Tim is often seen walking around campus, hanging out at the coffee shop, laughing with his friends, and, as he puts it, “investing time with the ladies.” Tim started smoking in high school and has never tried to kick the habit. He jokes about the “smoker’s cough” that has punctuated his conversations over the summer and start of the fall semester. Recently, the cough has been getting worse, his throat is scratchy, his head hurts, and he is tired all the time. Tim wonders if he has some long-lasting flu, though he hasn’t had a fever. He decides not to waste time with a doctor’s visit, but the cough starts keeping him up at night. In October, after a month of progressively worse coughing, he’s had enough; he heads to the campus clinic right after his morning classes.
The clinic physician notes the persistence and worsening of Tim’s cough and confirms that Tim has no fever. To rule out a bacterial infection, she orders a routine sputum culture (a test of the material coughed up from Tim’s lungs), which comes back negative. Tim is sent home with the advice to quit smoking.
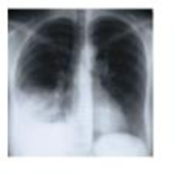
A week later, he’s back, coughing nonstop, short of breath, sweaty, and aching. A different doctor orders a chest X-ray exam and several blood tests. The X-ray film reveals fluid in Tim’s lungs, and real-time PCR confirms an infection with Mycoplasma pneumoniae, which is an atypical Gram-positive bacterium. Regular sputum microscopy doesn't detect this pathogen, which lacks cell walls and doesn’t stain well.
Mycoplasma pneumoniae infects and disrupts the mucous membranes of the lungs, invading and disrupting the epithelium. Pneumonia caused by M. pneumoniae is called “walking pneumonia” because the symptoms are often milder and come and go, making this disease different from streptococcal pneumonia. Most patients get better on their own, but not Tim. Smoke has compromised the lungs’ innate immunity. A course of an antimicrobial drug-azithromycin-clears Tim’s lungs of the bacterium within a week. Tim decides to quit smoking.
- 1. Which Toll-like receptors (TLRs) might have been involved in Tim’s innate immune response to Mycoplasma?
- 2. Why didn’t Tim’s naturally occurring interferons help clear the infection?
- 3. What structures and chemicals normally fend off lung infections?
- 4. Why didn’t Tim’s innate lung defenses operate properly?
Want to see the full answer?
Check out a sample textbook solution
Chapter 15 Solutions
Pearson eText Bauman Microbiology with Diseases by Body Systems -- Instant Access (Pearson+)


- Identify the indicated tissue. (Tilia stem x.s.) parenchyma collenchyma sclerenchyma xylem phloem none of thesearrow_forwardIdentify the indicated structure. (Cucurbita stem l.s.) pit lenticel stomate tendril none of thesearrow_forwardIdentify the specific cell? (Zebrina leaf peel) vessel element sieve element companion cell tracheid guard cell subsidiary cell none of thesearrow_forward
- What type of cells flank the opening on either side? (leaf x.s.) vessel elements sieve elements companion cells tracheids guard cells none of thesearrow_forwardWhat specific cell is indicated. (Cucurbita stem I.s.) vessel element sieve element O companion cell tracheid guard cell none of thesearrow_forwardWhat specific cell is indicated? (Aristolochia stem x.s.) vessel element sieve element ○ companion cell O O O O O tracheid O guard cell none of thesearrow_forward
- Identify the tissue. parenchyma collenchyma sclerenchyma ○ xylem O phloem O none of thesearrow_forwardPlease answer q3arrow_forwardRespond to the following in a minimum of 175 words: How might CRISPR-Cas 9 be used in research or, eventually, therapeutically in patients? What are some potential ethical issues associated with using this technology? Do the advantages of using this technology outweigh the disadvantages (or vice versa)? Explain your position.arrow_forward
- You are studying the effect of directional selection on body height in three populations (graphs a, b, and c below). (a) What is the selection differential? Show your calculation. (2 pts) (b) Which population has the highest narrow sense heritability for height? Explain your answer. (2 pts) (c) If you examined the offspring in the next generation in each population, which population would have the highest mean height? Why? (2 pts) (a) Midoffspring height (average height of offspring) Short Short Short Short (c) Short (b) Short Tall Short Tall Short Short Tall Midparent height (average height of Mean of population = 65 inches Mean of breading parents = 70 inches Mean of population = 65 inches Mean of breading parents = 70 inches Mean of population = 65 inches Mean of breading parents = 70 inchesarrow_forwardP You are studying a population of 100 flowers that has two alleles at a locus for flower color, blue (B) and green (G). There are 15 individuals with the BB genotype, 70 individuals with the BG genotype, and 15 individuals with the GG genotype. (a) What are the allele frequencies of B and G in the starting population? Show your calculations. (2 pts) (b) Is this population in Hardy-Weinberg equilibrium? Show your calculations. (3 pts) 12pt v Paragraph BIU UA AV & VT2V f CO Varrow_forwardIn a natural population of outbreeding plants, the variance of the total number of seeds per plant is 16. From the natural population, 20 plants are taken into the laboratory and developed into separate true-breeding lines by self- fertilization-with selection for high, low, or medium number of seeds-for 10 generations. The average variance in the tenth generation in each of the 20 sets is about equal and averages 5.8 across all the sets. Estimate the broad-sense heritability for seed number in this population. (4 pts) 12pt v Paragraph BIUA V V T² v B ① O wordsarrow_forward
 Medical Terminology for Health Professions, Spira...Health & NutritionISBN:9781305634350Author:Ann Ehrlich, Carol L. Schroeder, Laura Ehrlich, Katrina A. SchroederPublisher:Cengage Learning
Medical Terminology for Health Professions, Spira...Health & NutritionISBN:9781305634350Author:Ann Ehrlich, Carol L. Schroeder, Laura Ehrlich, Katrina A. SchroederPublisher:Cengage Learning
 Comprehensive Medical Assisting: Administrative a...NursingISBN:9781305964792Author:Wilburta Q. Lindh, Carol D. Tamparo, Barbara M. Dahl, Julie Morris, Cindy CorreaPublisher:Cengage Learning
Comprehensive Medical Assisting: Administrative a...NursingISBN:9781305964792Author:Wilburta Q. Lindh, Carol D. Tamparo, Barbara M. Dahl, Julie Morris, Cindy CorreaPublisher:Cengage Learning- Understanding Health Insurance: A Guide to Billin...Health & NutritionISBN:9781337679480Author:GREENPublisher:Cengage