
Videos
The Stealth Invader
Tim is often seen walking around campus, hanging out at the coffee shop, laughing with his friends, and, as he puts it, “investing time with the ladies.” Tim started smoking in high school and has never tried to kick the habit. He jokes about the “smoker’s cough” that has punctuated his conversations over the summer and start of the fall semester. Recently, the cough has been getting worse, his throat is scratchy, his head hurts, and he is tired all the time. Tim wonders if he has some long-lasting flu, though he hasn’t had a fever. He decides not to waste time with a doctor’s visit, but the cough starts keeping him up at night. In October, after a month of progressively worse coughing, he’s had enough; he heads to the campus clinic right after his morning classes.
The clinic physician notes the persistence and worsening of Tim’s cough and confirms that Tim has no fever. To rule out a bacterial infection, she orders a routine sputum culture (a test of the material coughed up from Tim’s lungs), which comes back negative. Tim is sent home with the advice to quit smoking.
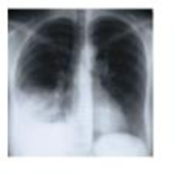
A week later, he’s back, coughing nonstop, short of breath, sweaty, and aching. A different doctor orders a chest X-ray exam and several blood tests. The X-ray film reveals fluid in Tim’s lungs, and real-time PCR confirms an infection with Mycoplasma pneumoniae, which is an atypical Gram-positive bacterium. Regular sputum microscopy doesn't detect this pathogen, which lacks cell walls and doesn’t stain well.
Mycoplasma pneumoniae infects and disrupts the mucous membranes of the lungs, invading and disrupting the epithelium. Pneumonia caused by M. pneumoniae is called “walking pneumonia” because the symptoms are often milder and come and go, making this disease different from streptococcal pneumonia. Most patients get better on their own, but not Tim. Smoke has compromised the lungs’ innate immunity. A course of an antimicrobial drug-azithromycin-clears Tim’s lungs of the bacterium within a week. Tim decides to quit smoking.
- 1. Which Toll-like receptors (TLRs) might have been involved in Tim’s innate immune response to Mycoplasma?
- 2. Why didn’t Tim’s naturally occurring interferons help clear the infection?
- 3. What structures and chemicals normally fend off lung infections?
- 4. Why didn’t Tim’s innate lung defenses operate properly?
Want to see the full answer?
Check out a sample textbook solution
Chapter 15 Solutions
EBK MICROBIOLOGY:W/DISEASES BY BODY...-


- C MasteringHealth MasteringNu × session.healthandnutrition-mastering.pearson.com/myct/itemView?assignment ProblemID=17396416&attemptNo=1&offset=prevarrow_forward10. Your instructor will give you 2 amino acids during the activity session (video 2-7. A. First color all the polar and non-polar covalent bonds in the R groups of your 2 amino acids using the same colors as in #7. Do not color the bonds in the backbone of each amino acid. B. Next, color where all the hydrogen bonds, hydrophobic interactions and ionic bonds could occur in the R group of each amino acid. Use the same colors as in #7. Do not color the bonds in the backbone of each amino acid. C. Position the two amino acids on the page below in an orientation where the two R groups could bond together. Once you are satisfied, staple or tape the amino acids in place and label the bond that you formed between the two R groups. - Polar covalent Bond - Red - Non polar Covalent boND- yellow - Ionic BonD - PINK Hydrogen Bonn - Purple Hydrophobic interaction-green O=C-N H I. H HO H =O CH2 C-C-N HICK H HO H CH2 OH H₂N C = Oarrow_forwardFind the dental formula and enter it in the following format: I3/3 C1/1 P4/4 M2/3 = 42 (this is not the correct number, just the correct format) Please be aware: the upper jaw is intact (all teeth are present). The bottom jaw/mandible is not intact. The front teeth should include 6 total rectangular teeth (3 on each side) and 2 total large triangular teeth (1 on each side).arrow_forward12. Calculate the area of a circle which has a radius of 1200 μm. Give your answer in mm² in scientific notation with the correct number of significant figures.arrow_forwardDescribe the image quality of the B.megaterium at 1000X before adding oil? What does adding oil do to the quality of the image?arrow_forwardWhich of the follwowing cells from this lab do you expect to have a nucleus and why or why not? Ceratium, Bacillus megaterium and Cheek epithelial cells?arrow_forward14. If you determine there to be debris on your ocular lens, explain what is the best way to clean it off without damaging the lens?arrow_forward11. Write a simple formula for converting mm to μm when the number of mm's is known. Use the variable X to represent the number of mm's in your formula.arrow_forward13. When a smear containing cells is dried, the cells shrink due to the loss of water. What technique could you use to visualize and measure living cells without heat-fixing them? Hint: you did this technique in part I.arrow_forward10. Write a simple formula for converting μm to mm when the number of μm's are known. Use the variable X to represent the number of um's in your formula.arrow_forward8. How many μm² is in one cm²; express the result in scientific notation. Show your calculations. 1 cm = 10 mm; 1 mm = 1000 μmarrow_forwardFind the dental formula and enter it in the following format: I3/3 C1/1 P4/4 M2/3 = 42 (this is not the correct number, just the correct format) Please be aware: the upper jaw is intact (all teeth are present). The bottom jaw/mandible is not intact. The front teeth should include 6 total rectangular teeth (3 on each side) and 2 total large triangular teeth (1 on each side).arrow_forwardarrow_back_iosSEE MORE QUESTIONSarrow_forward_ios
 Medical Terminology for Health Professions, Spira...Health & NutritionISBN:9781305634350Author:Ann Ehrlich, Carol L. Schroeder, Laura Ehrlich, Katrina A. SchroederPublisher:Cengage Learning
Medical Terminology for Health Professions, Spira...Health & NutritionISBN:9781305634350Author:Ann Ehrlich, Carol L. Schroeder, Laura Ehrlich, Katrina A. SchroederPublisher:Cengage Learning
 Comprehensive Medical Assisting: Administrative a...NursingISBN:9781305964792Author:Wilburta Q. Lindh, Carol D. Tamparo, Barbara M. Dahl, Julie Morris, Cindy CorreaPublisher:Cengage Learning
Comprehensive Medical Assisting: Administrative a...NursingISBN:9781305964792Author:Wilburta Q. Lindh, Carol D. Tamparo, Barbara M. Dahl, Julie Morris, Cindy CorreaPublisher:Cengage Learning- Understanding Health Insurance: A Guide to Billin...Health & NutritionISBN:9781337679480Author:GREENPublisher:Cengage